A nursing case study is a patient-based clinical analysis that explains how assessment, nursing judgment, care planning, and follow-up decisions work in a real situation. The usual writing process of a sample case study for nursing students includes:
- Choose a patient case with a distinct clinical diagnosis.
- Take a detailed patient history, including symptoms, tests, medications, and any other information about care
- Identify the nursing problems and possible nursing diagnoses.
- Document the interventions and the response of the patient, any outcomes, and any lessons that were learned.
In this guide, I will cover the purpose of the case study, common types, the structure of the document, and exactly how to write a nursing case study that reflects real care.
Why Should You Write a Nursing Case Study?
The purpose of case study in nursing is to help students develop clinical thinking skills through the various details of providing care to a patient. A case study requires you to think critically about your evidence-based practice and how you made your nursing decision in that specific situation. The reasons why you might need a nursing case study are to:
- Develop clinical reasoning skills using individual patient data.
- Make connections between symptoms, clinical findings, and nursing diagnoses.
- Increase your level of confidence in both care planning and documentation.
- Provide an interpretation of outcomes based on the evidence reviewed, the response of the patient to the provided care, and your interpretation of whether and how the nursing care was successful.
Make Your Paper Clearer
Get support with research, structure, citations, and editing.

Types of Case Studies in Nursing
While there are several types of nursing case studies, intrinsic, explanatory, illustrative, cumulative, and critical are the ones we see most often. Which one you select depends on the assignment guidelines, the patient's case, and the kind of clinical reasoning demonstrated in the writing.
Intrinsic Case Study
The intrinsic case study focuses on one patient and their case because of its uniqueness. The writer must focus on this one patient's history, past and present symptoms, care requirements, and response to treatment within a more or less narrow frame. Intrinsic case studies are best when the patient has a rare condition or a common one with unusual presentation, complex medical history, or a potential care path that will be less meaningful if it's not treated as a unique case.
Explanatory Case Study
An explanatory case study focuses on the reasons something changed, or generally happened, during care (e.g., Why were their symptoms worse than before? Why did a care plan result in an improvement? Why did an intervention not yield positive results?). The explanatory study is usually used in nursing because it encourages the writer to link clinical reasons with nursing decisions and patient outcomes.
Illustrative Case Study
This case study depicts a nursing concept in the context of an actual patient situation. The focus of an illustrative case study may include, but is not limited to, the following: patient education, wound care, fall risk prevention, medication teaching, discharge planning, or chronic disease management. For students, these case studies are often practical for understanding how familiar nursing concepts can be applied in real cases.
Cumulative Case Study
A cumulative case study allows the writer to examine multiple related patient cases together, typically, to identify patterns among experiences, care plans, and patient outcomes. In this type of study, for example, a nursing student could examine multiple patients with diabetes and compare and contrast the recurring issues regarding their blood glucose control, their education, compliance with medications, and/or follow-up care. The overall strength of this type comes through comparison, but the cases should also share a point of focus.
Critical Instance Case Study
A critical instance case study examines a serious event, decision, or point in the care of a patient that had clinical significance. It may deal with a safety issue, sudden clinical deterioration, ethical dilemma, emergency response, or communication failure. Careful judgment is required by the writer in this case because they have to explain what occurred, why what happened was of clinical importance, and what the situation revealed about nursing practice as a whole, teamwork, patient safety, and decision-making.
Benefits and Limitations of Case Study in Nursing
A case study for nursing students helps them visualize the reasoning behind caring for patients: the patient data, documentation of assessments, nursing interventions, and patient response, all within one document. The major disadvantage of using a case study is the fact that it is limited to one patient and their clinical situation.
Benefits
- Assists students in applying knowledge from the classroom to real-life situations with patients.
- Strengthens students' approach to assessments, documentation, and rationales for interventions.
- Assists in demonstrating how symptoms, risks, test results, and nursing diagnoses relate to each other.
- Motivates students to provide explanations for interventions, as opposed to simply identifying them.
- Allows students to practice care planning in a safer environment prior to becoming more independent in a clinical environment.
- Eases the discussion regarding outcomes because the evidence is already documented.
Limitations
- A single patient case cannot support a broad clinical conclusion by itself.
- If a patient’s data is incomplete, the analysis may not appear as strong as it originally did.
- The author's perceptions can influence the case if they stray from the evidence presented.
- Some authors will spend excessive time describing the patient and not enough time describing the actual nursing care.
- The Health Insurance Portability and Accountability Act (HIPAA) limits the details that can be documented.
Structure of a Nursing Case Study Paper
A clear nursing case study format gives the paper a workable order, which matters because nursing cases can become messy fast once symptoms, history, interventions, and outcomes all appear together. Most papers include these parts:
- Title page
- Abstract
- Case presentation
- Nursing assessment
- Care plan
- Implementation
- Evaluation
- Discussion
- Conclusion
- References
Title Page
The title page presents the basic academic background for the case study. It usually has the following information:
- Title of the paper
- Name of student
- Course name
- Instructor name
- Name of school
- Date submitted
Other programs may require the student's clinical placement, the case's treatment category, and/or the required citation style. The specific title should identify what the case study covers, e.g. “Case Study of a Patient With Type 2 Diabetes” instead of “Nursing Case Study.”
Abstract
The abstract gives the reader a brief overview of the entire case study before they read it. It should include the patient's main diagnosis, the primary nursing concern, the nursing care provided, and the overall outcome. Because this section is very short, you should state very little information regarding the patient's background. The reader does not require the entire history; only enough information to understand what the case involves and why it needs attention.
Case Presentation
The case presentation is an overview of the patient situation in a private, controlled manner. The case presentation may include: patient's age, sex, diagnosis, reason for admission, relevant history, current signs and symptoms, and the primary clinical issue. No identification details must be included here, even though the case will be more "complete" with these details present. The intent of this section is to provide enough information about the case to allow for clinical interpretation without turning the case into a typical medical record.
Nursing Assessment
The nursing assessment explains what the nurse observed, measured, reviewed, and documented. This part may include vital signs, pain level, mobility, mental status, medication use, lab results, nutrition status, skin condition, and the patient’s own concerns. A stronger assessment does more than place findings in a list. It explains which details matter most for care and how those details affect the nursing priorities.
Care Plan
The care plan connects the assessment findings with nursing action. This section usually includes nursing diagnoses, goals, interventions, and rationales. The goals need to be specific enough for later evaluation, because vague goals make the final outcome difficult to judge. For example, “improve mobility” gives little direction, while “patient will walk 20 meters with assistance by the end of the shift” gives a measurable target. Each intervention should clearly relate to the patient’s identified needs.
Implementation
The implementation section explains what care was actually provided. It may cover medication support, patient education, wound care, monitoring, safety measures, or communication with the healthcare team. This part should stay practical and precise. The reader should be able to understand what happened, who participated, and how the action addressed the nursing problem already described in the care plan.
Evaluation
The evaluation section reviews the patient’s response to care. This is where the writer explains if the patient’s pain decreased, breathing improved, wound status changed, mobility increased, or discharge understanding became clearer. The outcome should be compared with the goals set earlier in the paper. If a goal was only partly met, that should be stated directly, along with the likely reason and the next clinical step.
Discussion
The discussion section gives the paper more depth because it explains what the case shows about nursing practice. This may include patient safety, communication, clinical judgment, ethics, evidence-based care, or teamwork. The writer can also discuss what went well and what could have been handled more effectively. A discussion that only repeats the case presentation usually feels thin, so this part needs analysis, even if the analysis is brief.
Conclusion
The conclusion brings the case back to its main clinical lesson. It should restate the patient’s central issue, the nursing approach, and the outcome in a concise way. New evidence should stay out of this section. The reader should leave with a clear understanding of what the case demonstrated about nursing care and why that lesson is useful.
References
The references section lists every source used in the paper. These sources may include nursing textbooks, clinical guidelines, journal articles, care standards, and assigned course materials. Use the citation style required by the instructor, which is often APA in nursing programs. Every in-text citation should match a reference entry, and every reference entry should connect to a source used in the paper.
How to Prepare for Writing a Nursing Case Study?
Good preparation matters because a nursing case can become confusing once patient history, assessment findings, interventions, and outcomes all sit in the same draft. Before writing a nursing case study paper, you need to check the assignment, choose a patient case with enough clinical detail, organize the data, remove identifying information, and decide which nursing problem will guide the paper.
Review the Assignment First
Start with the assignment instructions, since they decide the limits of the paper more than personal preference does. Check the expected length, required headings, citation style, source requirements, and grading rubric. Nursing instructors may ask for similar case studies in very different formats, so the instructions should settle the structure early.
Choose a Clear Patient Case
Select a case that gives you enough clinical information to analyze, not just describe. A workable case usually includes a diagnosis, symptoms, nursing concerns, interventions, and some kind of patient response. If the available details are too thin, the paper may end up repeating the same basic facts.
Collect the Right Patient Data
Gather the patient history, assessment notes, medications, lab results, care details, and outcome information before drafting. It helps to group the information by category because scattered notes can make the case harder to control. This step also reduces the risk of nursing essay topics becoming long patient summaries with weak analysis.
Protect Patient Privacy
Remove names, exact dates, addresses, room numbers, and any detail that could identify the patient. General descriptors are enough for academic writing. Privacy is part of professional nursing practice, so the case should stay clinically useful without exposing personal information.
Identify the Main Nursing Focus
Choose the nursing problem that will carry the paper. Pain, impaired mobility, infection risk, poor glucose control, medication education, and discharge planning all lead to different care priorities. Once the focus is set, the assessment, care plan, and evaluation become easier to connect.
How to Write a Nursing Case Study?
Writing a nursing case study paper works best when the draft follows the same logic as the care process: patient context first, then assessment, nursing problem, care plan, intervention, outcome, and discussion. The paper should explain what happened in the case and why the nursing decisions made sense.
- Introduce the patient case. Give the patient’s age range, diagnosis, reason for care, and main clinical concern while keeping identifying details out. The reader needs enough context to understand the case, although the section should not read like a copied chart.
- Present the assessment findings. Include the symptoms, vital signs, patient complaints, lab results, medication information, and nursing observations that directly affect the case. Details that do not support the nursing focus can usually stay out.
- Identify the nursing problem. State the main nursing diagnosis or clinical concern, then connect it to the evidence already presented. This connection is important because the reader should see why that problem became the priority.
- Create the care plan. List the patient goals, nursing interventions, and rationales in a clear order. Goals need enough detail for later evaluation, since a vague goal makes the outcome hard to judge.
- Explain the implementation. Describe the care that was provided, including education, monitoring, safety measures, medication support, communication with the care team, or other relevant actions. This part should show what the nurse actually did.
- Evaluate the patient response. Compare the outcome with the goals in the care plan. State what improved, what remained unresolved, and what kind of care may be needed next.
- Write the discussion. Explain what the case shows about nursing judgment, patient safety, communication, evidence-based care, or patient education. This section should add analysis, because a case study with only facts feels unfinished.
- Add the references. Cite the textbooks, clinical guidelines, journal articles, and course materials used in the paper. The reference list should follow the required citation style and match the sources cited in the text.
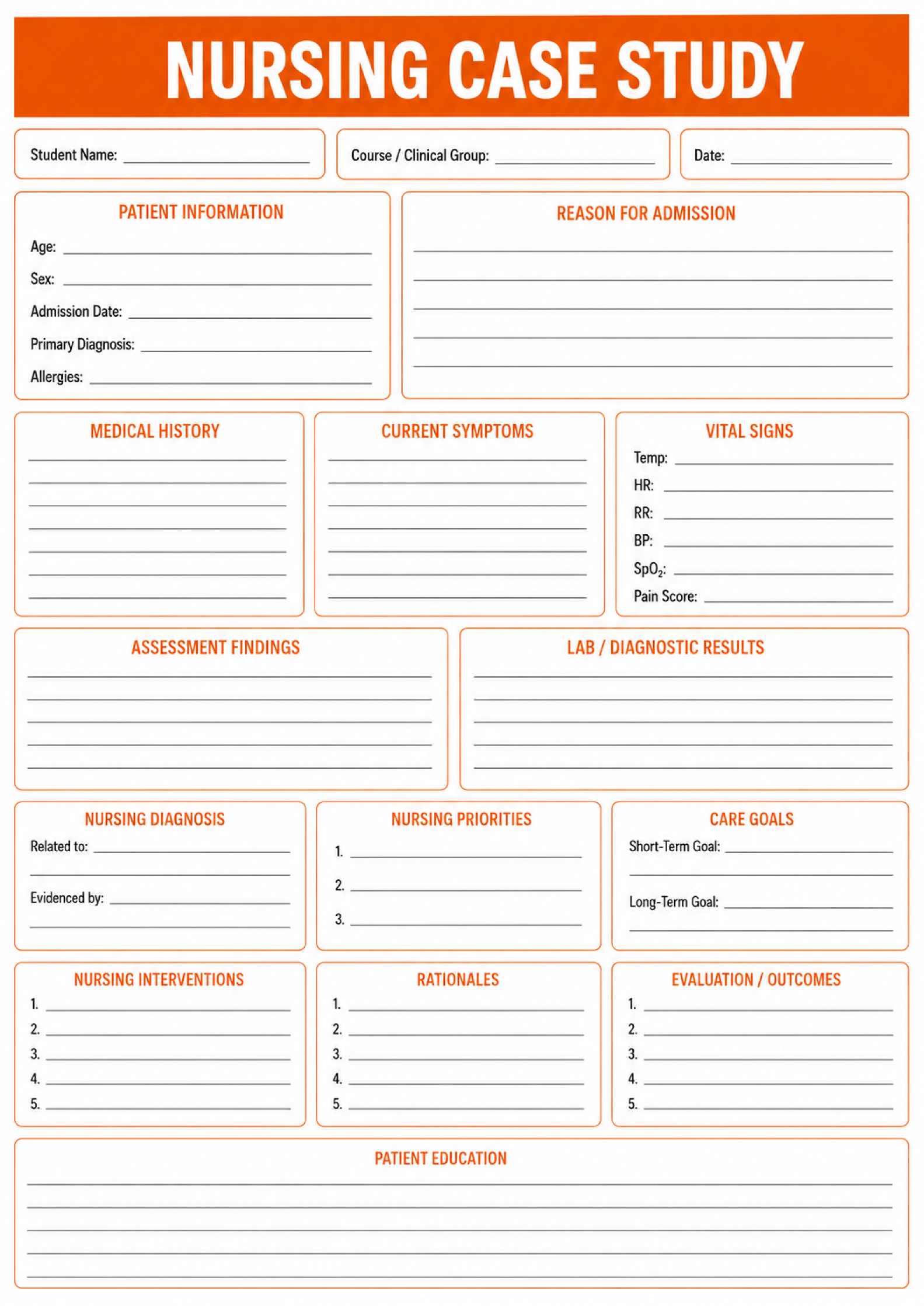
Standard Nursing Case Study Template
A nursing case study template should give the paper enough order that the reader can follow the clinical reasoning without feeling pushed through a rigid form. Usually, it moves through patient background, assessment, nursing diagnosis, care planning, interventions, outcomes, and reflection, although the exact layout may change by course. The template should guide the work, yes, but the student still has to make clinical decisions on the page.
Ethical Dilemmas & HIPAA Privacy in Nursing Case Studies
Nursing case study examples can help students understand structure, yet they can also create a false sense that patient details are safe once they appear in an academic assignment. They are not. Regardless of which nursing research topics you choose, a patient case still contains protected health information when it is used for class, and students have a legal and professional duty to remove identifying details before submission. If a student fails to protect a patient’s identity, the consequences can be serious: a failed assignment, suspension from the nursing program, or a legal HIPAA violation. That is not a technicality. It is part of safe nursing practice.
Before a case study is submitted, the de-identification process should be deliberate:
- Remove the patient’s full name, initials, address, phone number, email, and medical record number.
- Replace exact dates with general time references, such as “early in the admission” or “during the second week of care.”
- Leave out the hospital name, unit name, clinic name, physician name, nurse name, and family member names.
- Cut unusual personal details that could identify the patient indirectly.
- Use age ranges instead of exact ages unless the exact age is clinically necessary.
- Check images, forms, screenshots, lab reports, and copied notes for hidden identifiers.
- Ask the instructor or clinical supervisor before using any detail that feels uncertain.
Ethical conflicts need careful handling as well. If the case involves refusal of care, consent concerns, family disagreement, unsafe practice, or end-of-life decisions, the paper should describe the facts in a controlled and objective way. The analysis should rely on professional ethical codes, facility policy, and nursing standards. Personal reactions may explain why the situation felt difficult, and sometimes that context matters, but emotional bias should not become the basis for clinical judgment.
Submit With More Confidence
Our writing service helps students organize complex assignments and build papers that follow the requirements.

Nursing Case Study Examples
An example of a case study in nursing should read like clinical analysis, not a loose essay about a diagnosis. At this point, many aspiring nurses use SOAP notes to easily structure all information they gather. A strong example includes patient background, presenting symptoms, objective assessment findings, lab or diagnostic data, nursing priorities, interventions, rationales, and outcome evaluation. The case should feel specific enough to support nursing judgment while still protecting the patient’s identity.
Nursing Case Study Example #1: Community-Acquired Pneumonia
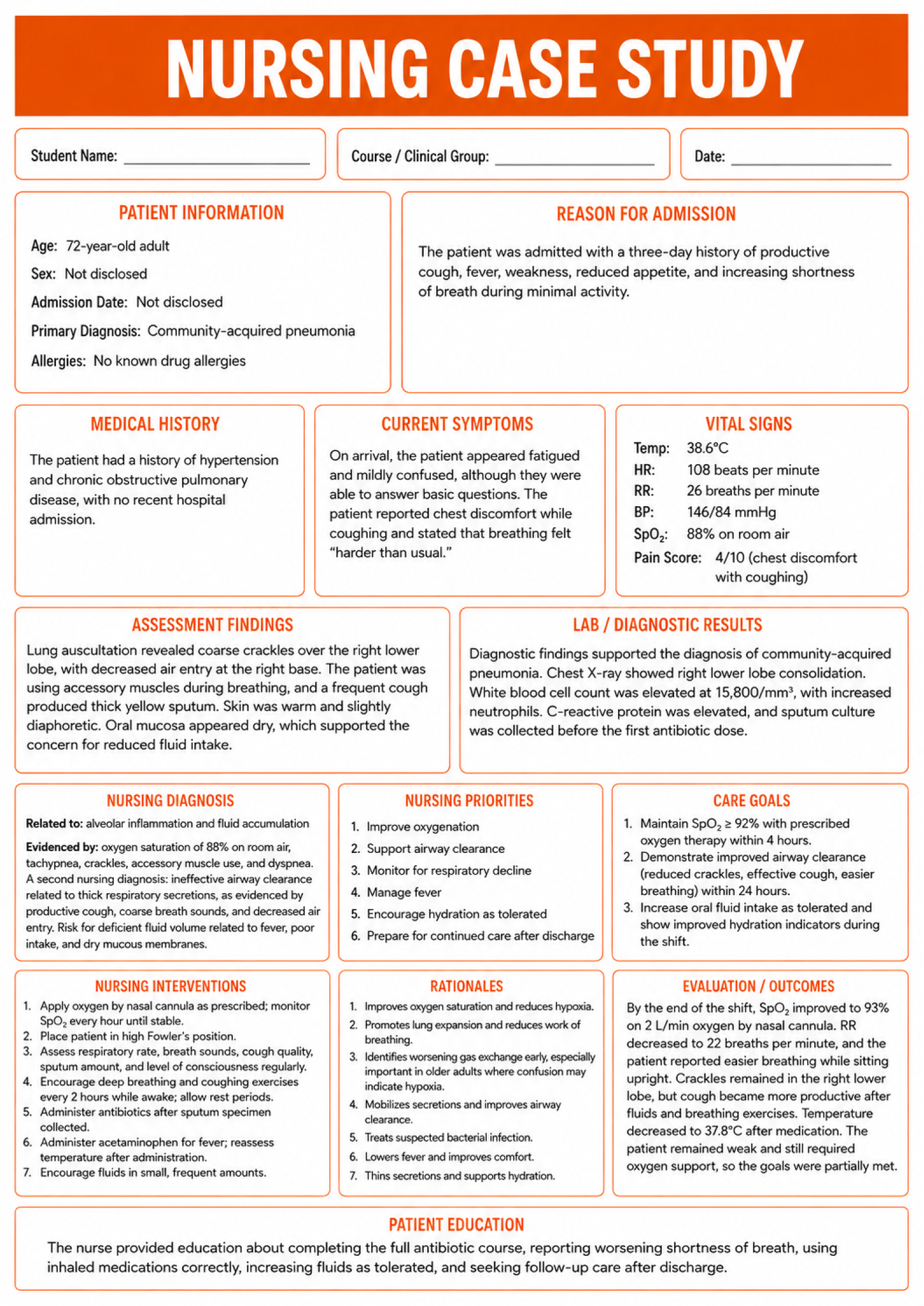
Patient Information
A 72-year-old adult patient was admitted to the medical unit. No identifying details, such as the patient’s name, hospital name, room number, exact admission date, or medical record number, are included.
Reason for Admission
The patient was admitted with a three-day history of productive cough, fever, weakness, reduced appetite, and increasing shortness of breath during minimal activity.
Medical History
The patient had a history of hypertension and chronic obstructive pulmonary disease. No recent hospital admission was reported.
Current Symptoms
On arrival, the patient appeared fatigued and mildly confused, although they were able to answer basic questions. The patient reported chest discomfort while coughing and stated that breathing felt “harder than usual.”
Vital Signs
- Temperature: 38.6°C
- Heart rate: 108 beats per minute
- Respiratory rate: 26 breaths per minute
- Blood pressure: 146/84 mmHg
- Oxygen saturation: 88% on room air
Assessment Findings
Lung auscultation revealed coarse crackles over the right lower lobe, with decreased air entry at the right base. The patient was using accessory muscles during breathing. A frequent cough produced thick yellow sputum. Skin was warm and slightly diaphoretic. Oral mucosa appeared dry, which supported the concern for reduced fluid intake.
Lab / Diagnostic Results
Diagnostic findings supported community-acquired pneumonia. Chest X-ray showed right lower lobe consolidation. White blood cell count was elevated at 15,800/mm³, with increased neutrophils. C-reactive protein was elevated. A sputum culture was collected before the first antibiotic dose.
Nursing Diagnosis
The priority nursing diagnosis was impaired gas exchange related to alveolar inflammation and fluid accumulation, as evidenced by oxygen saturation of 88% on room air, tachypnea, crackles, accessory muscle use, and dyspnea.
A second nursing diagnosis was ineffective airway clearance related to thick respiratory secretions, as evidenced by productive cough, coarse breath sounds, and decreased air entry.
Risk for deficient fluid volume was also relevant because of fever, poor intake, and dry mucous membranes.
Nursing Priorities
The main nursing priorities were improving oxygenation, supporting airway clearance, monitoring for respiratory decline, managing fever, encouraging fluids as tolerated, and preparing the patient for safe follow-up care after discharge.
Care Goals
The first nursing goal was for the patient to maintain oxygen saturation at or above 92% with prescribed oxygen therapy within four hours.
Another goal was for the patient to demonstrate improved airway clearance through more effective coughing, reduced crackles, and easier breathing within 24 hours.
A third goal was for the patient to increase oral fluid intake as tolerated and show improved hydration indicators during the shift.
Nursing Interventions
Nursing interventions included applying oxygen by nasal cannula as prescribed and monitoring oxygen saturation every hour until stable. The nurse placed the patient in high Fowler’s position. Respiratory rate, breath sounds, cough quality, sputum amount, and level of consciousness were assessed regularly.
The nurse encouraged deep breathing and coughing exercises every two hours while awake, with rest periods between activities. Antibiotics were administered after the sputum specimen had been collected. Acetaminophen was given for fever, and temperature was reassessed after administration. Fluids were encouraged in small, frequent amounts as tolerated.
Rationales
Oxygen therapy was used to improve oxygen saturation and reduce hypoxia. High Fowler’s position helped improve lung expansion and reduce the work of breathing. Regular respiratory assessment was necessary because worsening hypoxia can appear first as confusion in older adults. Deep breathing and coughing helped mobilize secretions. Antibiotics treated the suspected bacterial infection, while fluids helped loosen secretions and support hydration.
Evaluation / Outcomes
By the end of the shift, the patient’s oxygen saturation improved to 93% on 2 L/min oxygen by nasal cannula. Respiratory rate decreased to 22 breaths per minute, and the patient reported that breathing felt easier while sitting upright.
Crackles remained present in the right lower lobe, although cough became more productive after fluids and breathing exercises. Temperature decreased to 37.8°C after medication. The patient remained weak and still required oxygen support, so the goals were partially met. Continued monitoring, antibiotic therapy, airway clearance support, hydration management, and patient education remained necessary.
Patient Education
The nurse provided education about completing the full antibiotic course, reporting worsening shortness of breath, using inhaled medications correctly, and seeking follow-up care after discharge.
References
No references are listed in this brief example. In a full nursing case study paper, this section should include clinical guidelines, nursing textbooks, journal articles, and course materials used to support the care plan.
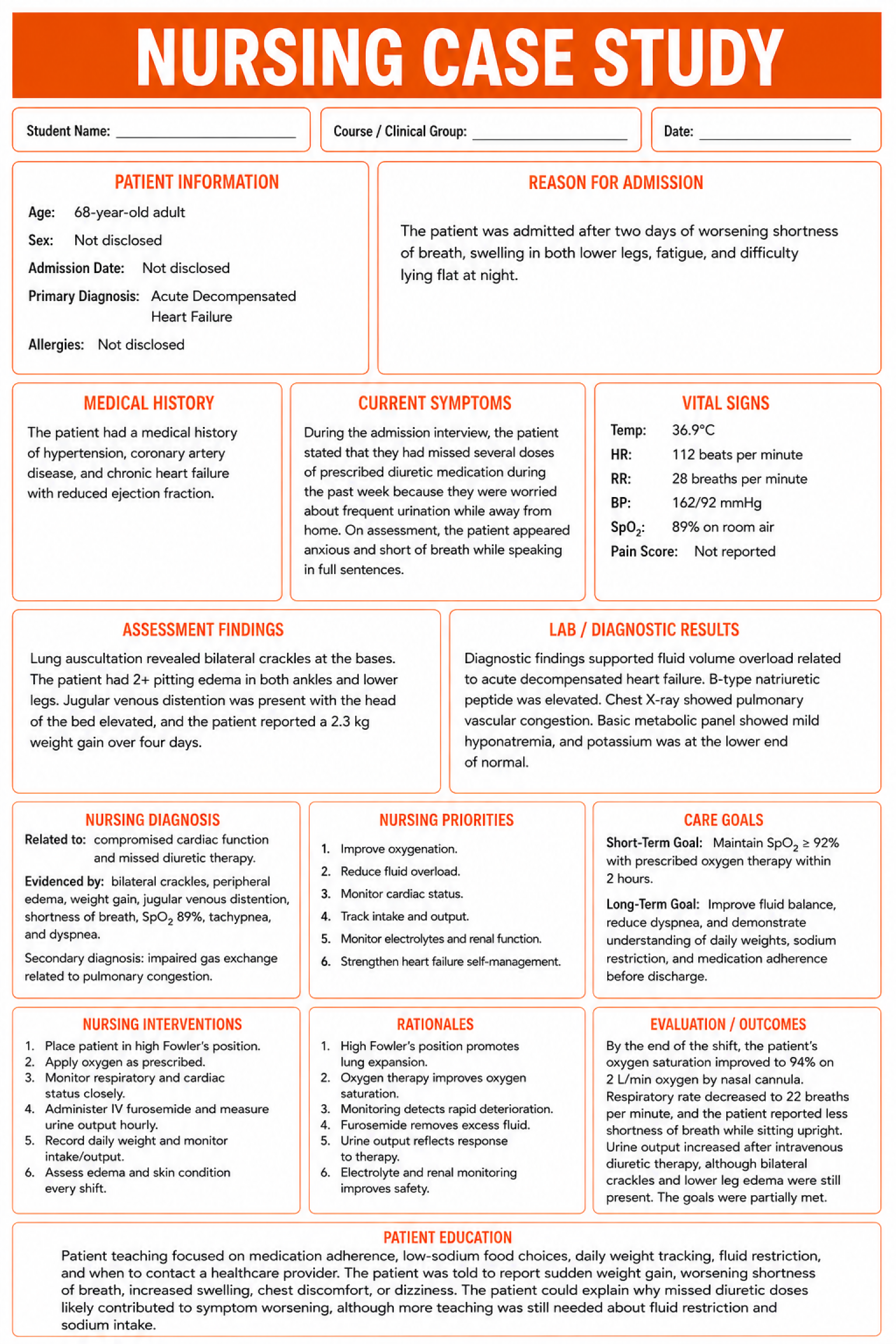
Nursing Case Study Example #2: Acute Decompensated Heart Failure
Patient Information
A 68-year-old adult patient was admitted to the cardiac unit. No identifying details, such as the patient’s name, hospital name, room number, exact admission date, or medical record number, are included.
Reason for Admission
The patient was admitted after two days of worsening shortness of breath, swelling in both lower legs, fatigue, and difficulty lying flat at night.
Medical History
The patient had a medical history of hypertension, coronary artery disease, and chronic heart failure with reduced ejection fraction.
Current Symptoms
During the admission interview, the patient stated that they had missed several doses of prescribed diuretic medication during the past week because they were worried about frequent urination while away from home. On assessment, the patient appeared anxious and short of breath while speaking in full sentences.
Vital Signs
- Blood pressure: 162/92 mmHg
- Heart rate: 112 beats per minute
- Respiratory rate: 28 breaths per minute
- Oxygen saturation: 89% on room air
- Temperature: 36.9°C
Assessment Findings
Lung auscultation revealed bilateral crackles at the bases. The patient had 2+ pitting edema in both ankles and lower legs. Jugular venous distention was present with the head of the bed elevated. The patient also reported a 2.3 kg weight gain over four days.
Lab / Diagnostic Results
Diagnostic findings supported fluid volume overload related to acute decompensated heart failure. B-type natriuretic peptide was elevated. Chest X-ray showed pulmonary vascular congestion. Basic metabolic panel showed mild hyponatremia, and potassium was at the lower end of normal.
Nursing Diagnosis
The priority nursing diagnosis was excess fluid volume related to compromised cardiac function and missed diuretic therapy, as evidenced by bilateral crackles, peripheral edema, weight gain, jugular venous distention, and shortness of breath.
A second nursing diagnosis was impaired gas exchange related to pulmonary congestion, as evidenced by oxygen saturation of 89% on room air, tachypnea, dyspnea, and bilateral crackles.
Nursing Priorities
The main nursing priorities were improving oxygenation, reducing fluid overload, monitoring cardiac status, tracking intake and output, checking renal function and electrolytes, and helping the patient understand heart failure self-management.
Care Goals
The first goal was for the patient to maintain oxygen saturation at or above 92% with prescribed oxygen therapy within two hours.
Another goal was for the patient to show improved fluid balance through increased urine output, reduced dyspnea, and stable vital signs during the shift.
A longer-term goal was for the patient to explain the purpose of daily weights, diuretic adherence, and sodium restriction before discharge.
Nursing Interventions
Nursing interventions included placing the patient in high Fowler’s position and applying oxygen as prescribed. Oxygen saturation, respiratory rate, lung sounds, heart rhythm, blood pressure, and level of distress were monitored closely.
The nurse administered intravenous furosemide and measured urine output hourly after administration. Daily weight was recorded using the same scale, and intake and output were documented carefully.
The nurse also monitored potassium and renal function. Edema was assessed during each shift, with attention to changes in swelling and skin condition.
Rationales
High Fowler’s position helped reduce the work of breathing and supported lung expansion. Oxygen therapy was used to improve low oxygen saturation caused by pulmonary congestion. Close respiratory and cardiac monitoring was necessary because heart failure symptoms can worsen quickly.
Intravenous furosemide helped remove excess fluid, while hourly urine output showed the patient’s response to diuretic therapy. Daily weights and intake and output records helped track fluid balance. Potassium and renal function monitoring were important because diuretic therapy can affect electrolyte balance and kidney perfusion.
Evaluation / Outcomes
By the end of the shift, the patient’s oxygen saturation improved to 94% on 2 L/min oxygen by nasal cannula. Respiratory rate decreased to 22 breaths per minute, and the patient reported less shortness of breath while sitting upright.
Urine output increased after intravenous diuretic therapy, although bilateral crackles and lower leg edema were still present. The goals were partially met. The patient showed early improvement in oxygenation and fluid removal, although continued monitoring remained necessary because signs of overload had not fully resolved.
Patient Education
Patient teaching focused on medication adherence, low-sodium food choices, daily weight tracking, fluid restriction, and when to contact a healthcare provider. The patient was told to report sudden weight gain, worsening shortness of breath, increased swelling, chest discomfort, or dizziness.
The patient could explain why missed diuretic doses likely contributed to symptom worsening, although more teaching was still needed about fluid restriction and sodium intake.
References
No references are listed in this brief example. In a full nursing case study paper, this section should include clinical guidelines, nursing textbooks, journal articles, cardiac care standards, and course materials used to support the care plan.
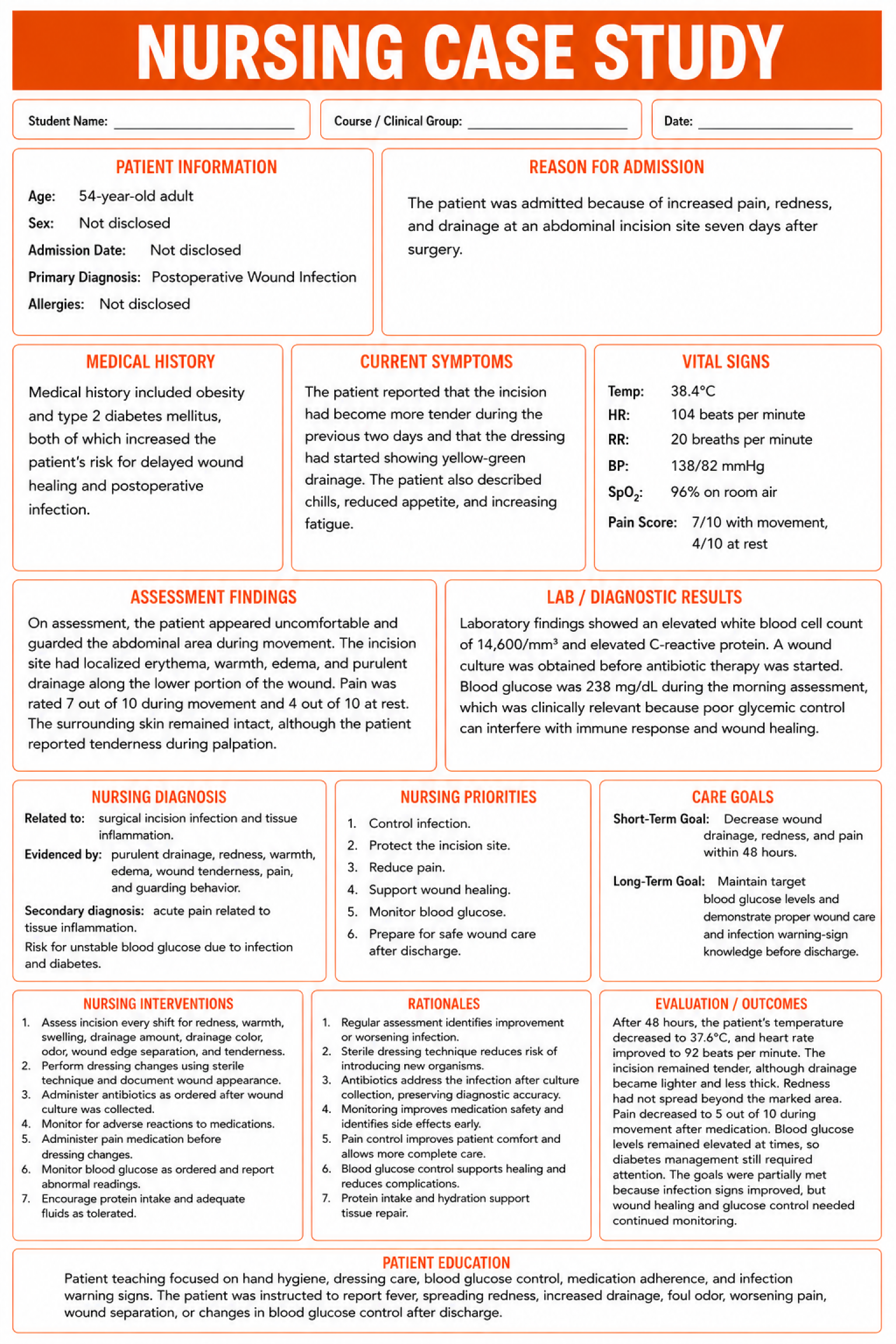
Nursing Case Study Example #3: Postoperative Wound Infection
Patient Information
A 54-year-old adult patient was admitted for evaluation after a recent open cholecystectomy. No identifying details, such as the patient’s name, hospital name, room number, exact admission date, or medical record number, are included.
Reason for Admission
The patient was admitted for evaluation of increased pain, redness, and drainage at an abdominal incision site seven days after surgery.
Medical History
Medical history included obesity and type 2 diabetes mellitus. Both conditions increased the risk for delayed wound healing and postoperative infection.
Current Symptoms
The patient reported that the incision had become more tender during the previous two days and that the dressing had started showing yellow-green drainage. The patient also described chills, reduced appetite, and increasing fatigue.
Vital Signs
- Temperature: 38.4°C
- Heart rate: 104 beats per minute
- Respiratory rate: 20 breaths per minute
- Blood pressure: 138/82 mmHg
- Oxygen saturation: 96% on room air
Assessment Findings
On assessment, the patient appeared uncomfortable and guarded the abdominal area during movement. The incision site had localized erythema, warmth, edema, and purulent drainage along the lower portion of the wound. Pain was rated 7 out of 10 during movement and 4 out of 10 at rest. The surrounding skin remained intact, although the patient reported tenderness during palpation.
Lab / Diagnostic Results
Laboratory findings showed an elevated white blood cell count of 14,600/mm³ and elevated C-reactive protein. A wound culture was obtained before antibiotic therapy was started. Blood glucose was 238 mg/dL during the morning assessment, which was clinically relevant because poor glycemic control can interfere with immune response and wound healing.
Nursing Diagnosis
The priority nursing diagnosis was impaired skin integrity related to surgical incision infection, as evidenced by purulent drainage, redness, warmth, edema, and increased wound pain.
A second nursing diagnosis was acute pain related to tissue inflammation, as evidenced by the patient’s pain rating, guarding, and limited movement.
Risk for unstable blood glucose was also important because infection can raise glucose levels and complicate healing.
Nursing Priorities
The main nursing priorities were controlling infection, protecting the incision site, reducing pain, monitoring blood glucose, supporting wound healing, and preparing the patient for safe wound care after discharge.
Care Goals
The first goal was for the patient’s wound drainage, redness, and pain to decrease during the next 48 hours.
Another goal was for the patient to maintain blood glucose within the ordered target range during hospitalization.
A third goal was for the patient to explain proper wound care and infection warning signs before discharge.
Nursing Interventions
Nursing interventions included assessing the incision site every shift for redness, warmth, swelling, drainage amount, drainage color, odor, wound edge separation, and increased tenderness.
The nurse performed dressing changes using sterile technique and documented wound appearance after each change. Antibiotics were administered as ordered after the wound culture was collected, and the patient was monitored for adverse reactions. Pain medication was given before dressing changes to reduce discomfort and allow more complete wound care.
Blood glucose was monitored as ordered, and abnormal readings were reported according to facility protocol. The nurse encouraged protein intake and adequate fluids as tolerated.
Rationales
Regular wound assessment helped track the infection and identify any worsening signs. Sterile dressing changes reduced the risk of introducing new organisms into the incision site. Antibiotics addressed the suspected infection after culture collection, which helped preserve diagnostic accuracy.
Pain medication before dressing changes improved comfort and allowed the nurse to complete wound care more effectively. Blood glucose monitoring was necessary because infection can raise glucose levels, and poor glycemic control can delay healing. Protein intake and adequate fluids supported tissue repair.
Evaluation / Outcomes
After 48 hours, the patient’s temperature decreased to 37.6°C, and heart rate improved to 92 beats per minute. The incision remained tender, although drainage became lighter and less thick. Redness had not spread beyond the marked area.
Pain decreased to 5 out of 10 during movement after medication. Blood glucose levels remained elevated at times, so diabetes management still required attention. The goals were partially met because infection signs improved, but wound healing and glucose control needed continued monitoring.
Patient Education
Patient teaching focused on hand hygiene, dressing care, blood glucose control, medication adherence, and warning signs such as fever, spreading redness, increased drainage, foul odor, or worsening pain. The patient was also prepared for safe discharge care and instructed to report changes promptly.
References
No references are listed in this brief example. In a full nursing case study paper, this section should include clinical guidelines, nursing textbooks, journal articles, surgical wound care standards, diabetes care sources, and course materials used to support the care plan.
If you still want to have a professional handle your papers because of the endless shifts and draining energy, our nursing essay writing service can step in whenever you request.
Final Thoughts
Writing a nursing case study means turning patient information into clear clinical reasoning. The strongest papers do more than describe a diagnosis. They connect assessment findings, nursing priorities, interventions, outcomes, and ethical responsibility. Keep the structure organized, protect patient privacy, and explain each decision with evidence. That is what makes the case useful, credible, and genuinely clinical.
FAQs
- Hensel, D. (n.d.). How to Write Case Study Questions Learning Objectives. https://www.nursing.umaryland.edu/media/son/mnwc/2021next-gen-nclex/Handout-slide-notes-pages.pdf
- How to Write a Case Study | NCEH | CDC. (2021, May 17). https://www.cdc.gov/. https://www.cdc.gov/nceh/clearwriting/case_study_guide.html
- Dr Brian Budgell. (2008). Guidelines to the writing of case studies. The Journal of the Canadian Chiropractic Association, 52(4), 199. https://pmc.ncbi.nlm.nih.gov/articles/PMC2597880/